Pekka Buttler, June 2021
Introduction
‘Comatic aberration’, most often referred to simply as ‘coma’, is one of those many failings that lens reviewers tend to test and mention. Too bad therefore, that a lot of them do not know what the heck they are talking about.
This article is part of a JAPB series of articles on the optical flaws of lenses and you can find the index of the series here.
What is coma? What is not coma?
First, we need to get one thing out of the way, because a lot of people seem to be confused about what coma is. I won’t point any fingers, but in my experience, a majority of lens reviews (and reviewers) out there who say that they are testing for ‘coma’ are actually finding something else.
They might, for instance, say that they find a lens to produce a lot of coma But when you look the pictures they show to back up their claims, what the pictures show is not coma but astigmatism, maybe with some coma thrown in. In some ways this mix-up is understandable, even somewhat forgivable, because – while being caused by quite different reasons, coma and astigmatism often plague the same kinds of shots and the remedy is often also similar.
Coma and astigmatism are phenomena that tend to plague nighttime, outdoors shots. Such shots are typically characterised by that most of the frame is very dark, even effectively black, but at the same time there are a number of bright, point-sources of light. There point-sources can be either distant streetlights, illuminated windows, or stars.
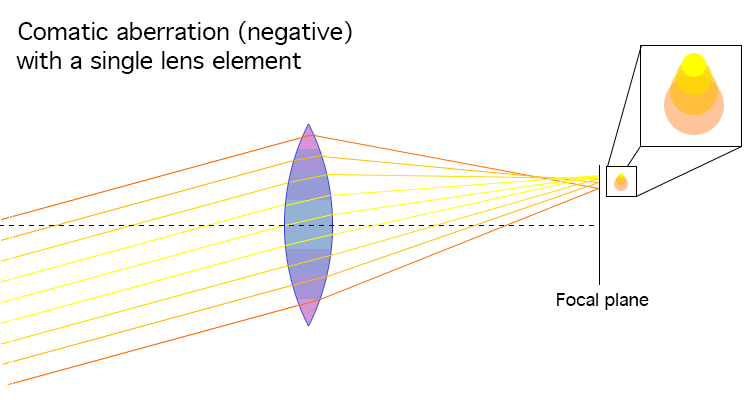
When those light-points are rendered as if each of them was trailing a monochromatic cone of diminishing illumination (a ‘comet’s tail’), and all those cones point either towards the image centre (more usual) or away from the image centre (less usual), then we’re talking about coma or comatic (≈comet-like) aberration. If, OTOH the point-source has some other weird affliction (traffic lights for martians, accretion disks, petals or wings or some combination of these, we’re not really talking about coma as such. See quick guide to aberrations of point light sources below:
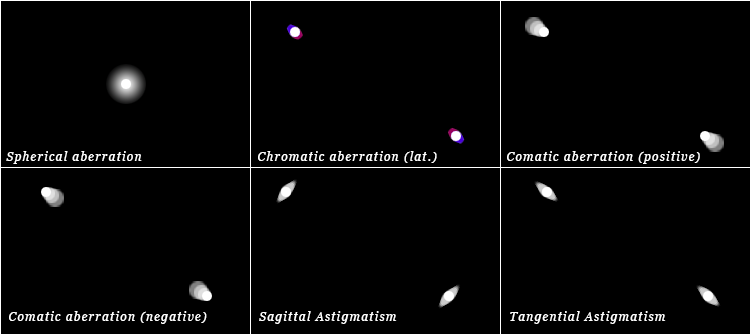
While Tangential Astigmatism may hide the simultaneous existence of Coma, Coma often combines with Sagittal Astigmatism.
What causes coma?
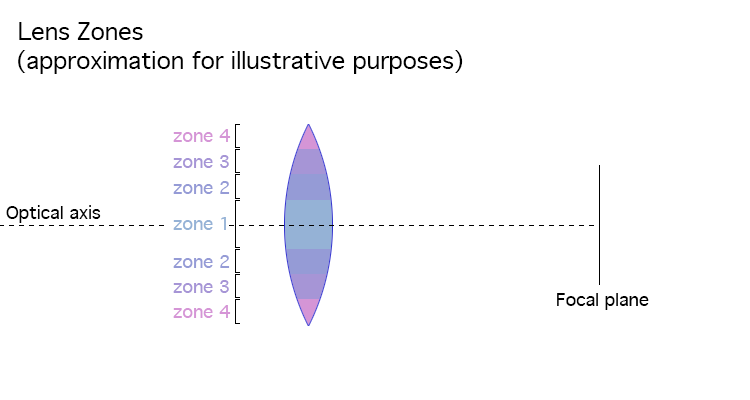
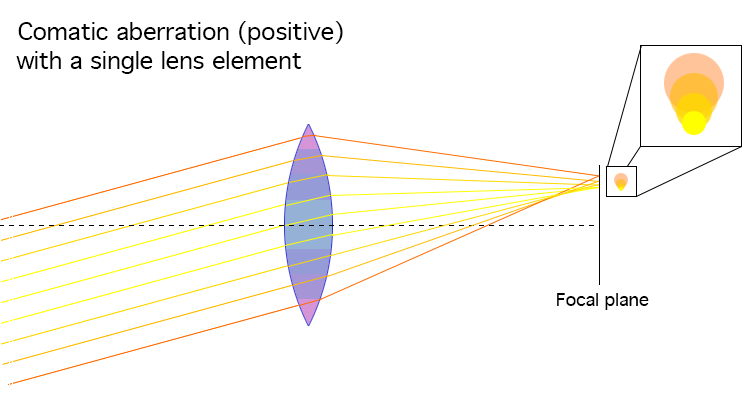
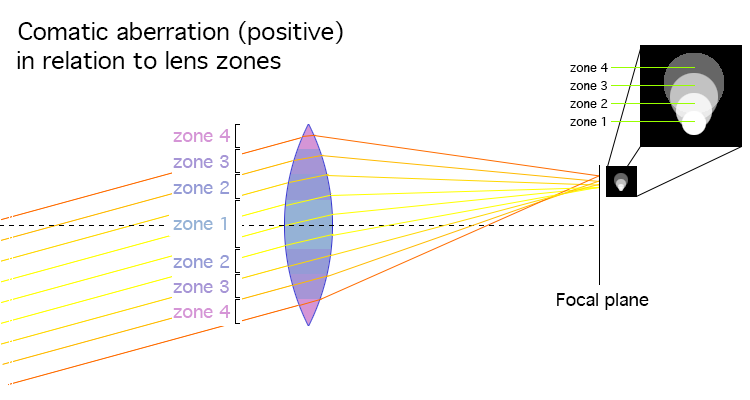
Coma is similar to spherical aberration in that they are both caused by how incoming parallel rays are refracted differently depending on what zone of the lens the rays strike. At the same time there are marked differences in that whereas spherical aberration causes some of each light point’s light to be spread around the main point of focus (causing an airy disk around the main light point), with coma that spreading around happens so that the airy disk is shifted – either away from the optical axis or toward the optical axis. To help illustrate the interaction see illustrations below, which depict an optical system that produces comatic aberration (not all optical systems do, obviously);
Why do some lenses have coma and others do not?
Again, a lens (objective) is the sum of its parts, i.e. the lens elements. If one element introduces an aberration, and another lens element is not added to correct that aberration, the entire lens will produce that aberration (and, potentially, others). Most often when a lens that produces visible coma, one or two lens elements are the main culprits.
If you search for “what causes coma[tic aberration]”, you are sure to encounter a phrase like: “[coma] is caused by the curvature of the principal planes of the optical system.”, which – unless you know the jargon and the secret handshake – is not really helpful. The main point is that a lens element’s propensity to produce coma is dependent on a combination of the angle of incoming rays (vs. the optical axis) and the shape of the lens element, especially, it’s forward-facing side. For example, a plano-convex lens is liable to produce mild negative comatic aberration when its flat side is facing the incoming rays, whereas when it’s turned the other way around (‘convex-plano’), it will produce positive comatic aberration. Also, as a general rule, large aperture lenses have a tendency to produce more visible coma (think: zones farther off-axis).
But the short story is that lens design is a game of making choices and accepting trade-offs. And given that some of those same lens element forms that are liable to lead to coma are very useful, the lens designer will either:
– have to accept a lens that produces coma,
– make adjustments to the design to reduce coma, simultaneously worsening other aberrations, or
– introduce extra elements to compensate for coma, thus increasing lens size, complexity, and price.
I don’t shoot astro, or night-time vistas. Why should I care about coma?
Well, first: you should care about coma. Not necessarily more than other aberrations, but care you should. The reason is simple.
While you need a wide-open shot of a night-time vista or a starlit sky to see the coma-like pattern clearly (thus helping you diagnose that the lens, indeed, produces coma), that does not mean that you would not have coma in every wide-open shot. Just as with all other aberrations that become clearly visible in specific circumstances (like spherical aberration or astigmatism in point-light sources or chromatic aberration in high-contrast transitions), coma is not just a pain in extreme-contrast shots. Instead, if the lens produces coma in starlit nights, it will produce coma also in regluar, low contrast situations. Coma, just as spherical aberration, leads to an overall lessening of contrast and definition, with two qualifications:
Firstly, given that coma does not occur with rays that come in along the optical axis, coma cannot occur in the centre of the frame (spherical aberration, however, can). At the same time, for rays to be liable to produce coma (in combination with ‘suitable’ lens elements), those rays do not need to be especially oblique – even tele lenses and telescopes can suffer coma.
Secondly, while one needs to photograph a starlit sky (or similar extreme contrast setting with point-light sources) to be able to distinguish between coma, astigmatism, spherical aberration and field curvature with certainty, coma – especially when strong – is liable to not only produce a general lessening of definition and contrast, but may (similarly to tangential astigmatism and field curvature) contribute to an image that looks like the corners are stretched-out or smeared1.
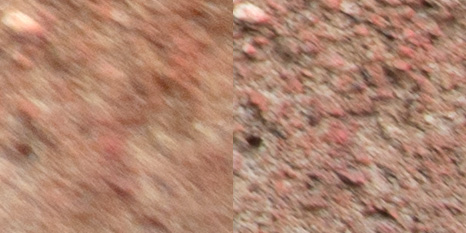
– Left: lens wide open (f/2) and corrected for vignetting;
– Right: lens stopped down (f/5.6);
Notice clear streaking/directionality in left sample.
Dealing with coma in the field.
Considering the mechanism that causes coma, the field-relevant remedy is obvious: stopping down the lens. The next question – stop down by how much? – however is harder to answer as lens designs vary strongly. My field experience is that a large majority of lenses that show visible coma wide open will show no field-relevant coma after stopping down two stops. Moreover, what is especially heartening is that with most lenses coma will be significantly reduced even after stopping down one stop. There are, however, exceptions and the only way one can make sure is to test one’s lens.
Problematically, your key reason for getting a large aperture lens may be your intent to use it wide open, either to facilitate handheld shooting, or to be able to shoot starlit skies without either having to raise your camera’s sensitivity too much (or having to invest in a equatorial mount system), and in such cases you’ll not be satisfied with a lens unless it is coma-free wide open (or stopped down by less than a stop).
Footnotes
1 I want to emphasise that stretching-out/smearing of corners may have many causes (coma, tangential astigmatism, field curvature), and an unequivocal diagnosis of smearing can never be made based just on one shot.
Read more:
• https://www.olympus-lifescience.com/en/microscope-resource/primer/java/aberrations/coma/
• https://www.azooptics.com/Article.aspx?ArticleID=660
• http://electron6.phys.utk.edu/optics421/modules/m2/aberration.htm